From “Mother’s Little Helper” to Ozempic: The History of Female Pharmaceutical Culture
I searched ‘Ozempic’ on Instagram looking for a quote to start this article. Before I even began scrolling, there was a message pinned to the top of the reels: “Your well-being is important. If you find yourself thinking a lot about weight or eating habits, these resources may help.” Underneath was a button linking to a page filled with reassuring phrases like “Know that your body is good enough.” and “Take care of yourself.”
I couldn’t help but laugh.
For centuries, women have been told, pressured and medicated into fitting social expectations, and here we are in 2026 facing many of the same problems. The difference is that now there’s a small warning label attached, almost patronising in tone, as if that could somehow counteract the millions of toxic messages hurled at women every day from every conceivable angle.
Throughout history we’ve been sold a magic pill to fix women’s problems. Sometimes those pills weren’t even treating problems at all. Sometimes they didn’t fix anything. And as a society, we can never seem to decide whether women are supposed to take them. Certain drugs are practically encouraged – Ozempic being a contemporary example – while others remain tinged with shame, like antidepressants.
So, as I often do, I found myself turning to history and asking a simple question: what makes one drug socially acceptable and another shameful, and why does it never seem to be women who decide this?
In this post I’ll look at three different eras as case studies: the 1950s, the 1960s and 1990s. I’m not talking about psychedelics or LSD, the drugs that tend to be glamourised in discussions of the 1960s or 1990s. I’m interested in a different kind of drug culture: the widespread, everyday pharmaceutical culture that existed inside suburban medicine cabinets and disproportionately affected women.
1950s
To set the scene, we need to briefly acknowledge the century leading up to the 1950s. Pill culture did not emerge from nowhere. From Victorian diagnoses of hysteria to opium tonics, sedatives and eventually lobotomies, there was a long tradition of treating women’s distress as something to be managed, subdued or corrected. By the post-war years the methods had changed, but many of the assumptions remained. It was no longer enough for a woman to be confined to bed and kept quiet. She was expected to get up, smile, raise children, host dinner parties, maintain a slim figure and create the perfect home. Fortunately (or unfortunately depending on your perspective) the pharmaceutical industry had a pill for that too.
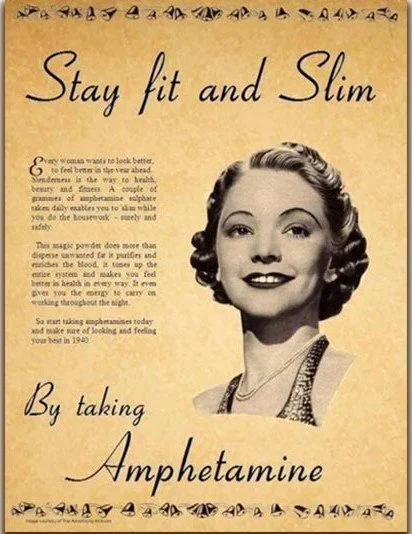
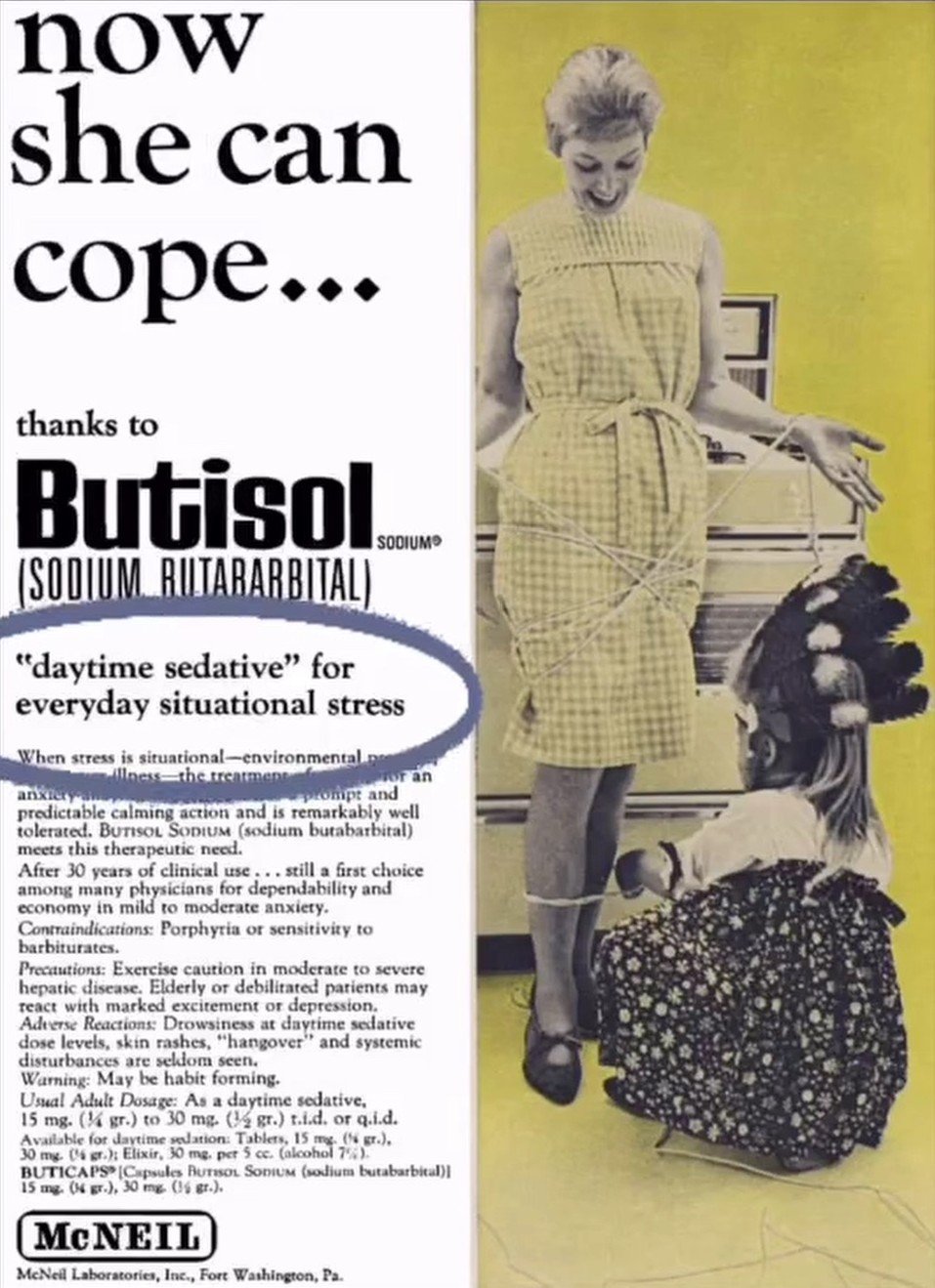
Historians often describe this period as the beginning of the ‘pharmaceutical management’ of everyday life, particularly for women. Housewives might be prescribed stimulant drugs such as Benzedrine to boost energy, barbiturates to help them sleep, sedatives for anxiety and amphetamine-based appetite suppressants for weight loss. Pep pills by day and sleeping pills by night. What a healthy cycle.
At this point, I should emphasise that not every woman was taking these medications. That caricature of the 1950s is neither accurate nor particularly useful. What matters is that seeking pharmaceutical solutions to everyday struggles was becoming increasingly normal, and increasingly encouraged. A woman did not need to be considered mentally ill to receive medication. She simply had to be struggling with the demands of modern womanhood.
What interests me most about this period is the tension between two competing narratives. The first is that women had these drugs imposed upon them, often by doctors, husbands, employers and wider social expectations. We can see traces of this narrative in the stories of Priscilla Presley, Marilyn Monroe and Judy Garland. The second comes from historians such as Andrea Tone, who argues that women were not merely passive victims of pharmaceutical culture. Many actively sought these medications because they offered genuine relief, even if broader social pressures were helping to create the demand in the first place.
If all of this sounds a little abstract, some of the most famous women of the 1950s provide striking case studies of feelings that were felt by many women during this period. Marilyn Monroe became highly reliant on prescription medication for sleep and anxiety while struggling under the pressures of fame, relentless scrutiny and the expectation that she remain forever beautiful, desirable and available. Years later, Priscilla Presley recalled being given amphetamines as a teenager to help maintain the appearance expected of her as Elvis Presley’s girlfriend. In both cases, the drugs were presented as solutions to problems created by the very systems these women were trying to navigate. The expectation was not that society should change, but that women should adapt to it’s demands. If they were exhausted, anxious, unable to sleep, or struggling to maintain the required image, there was increasingly a prescription for that.
Yet focussing only on celebrities risks missing the bigger story. Pharmaceutical advertisements like the one above aimed at housewives promised calmness, confidence, energy, weight loss and emotional stability. They rarely suggested liberation; instead they promised that women could better care for their husbands, children and homes. By the 1960s, the phenomenon had become so familiar that the Rolling Stones could satirise it in Mother’s Little Helper, a song about a suburban woman relying on prescription pills to cope with daily life.
The normalisation of both experiences is what makes this era so fascinating. When a mother is shown in a film, a song, or an autobiographical memoir casually swallowing a tablet before carrying on with the dinner, the moment isn’t necessarily signalling addiction or crisis. More often, it is signalling something else entirely: a culture in which medication had become part of the routine toolkit for performing femineity. What is so striking is that these women were not generally shamed for needing pharmaceutical help. In many cases it was actively encouraged by doctors, advertisers and wider society and many women sought it out themselves as Andrea Tone suggests.
1960s
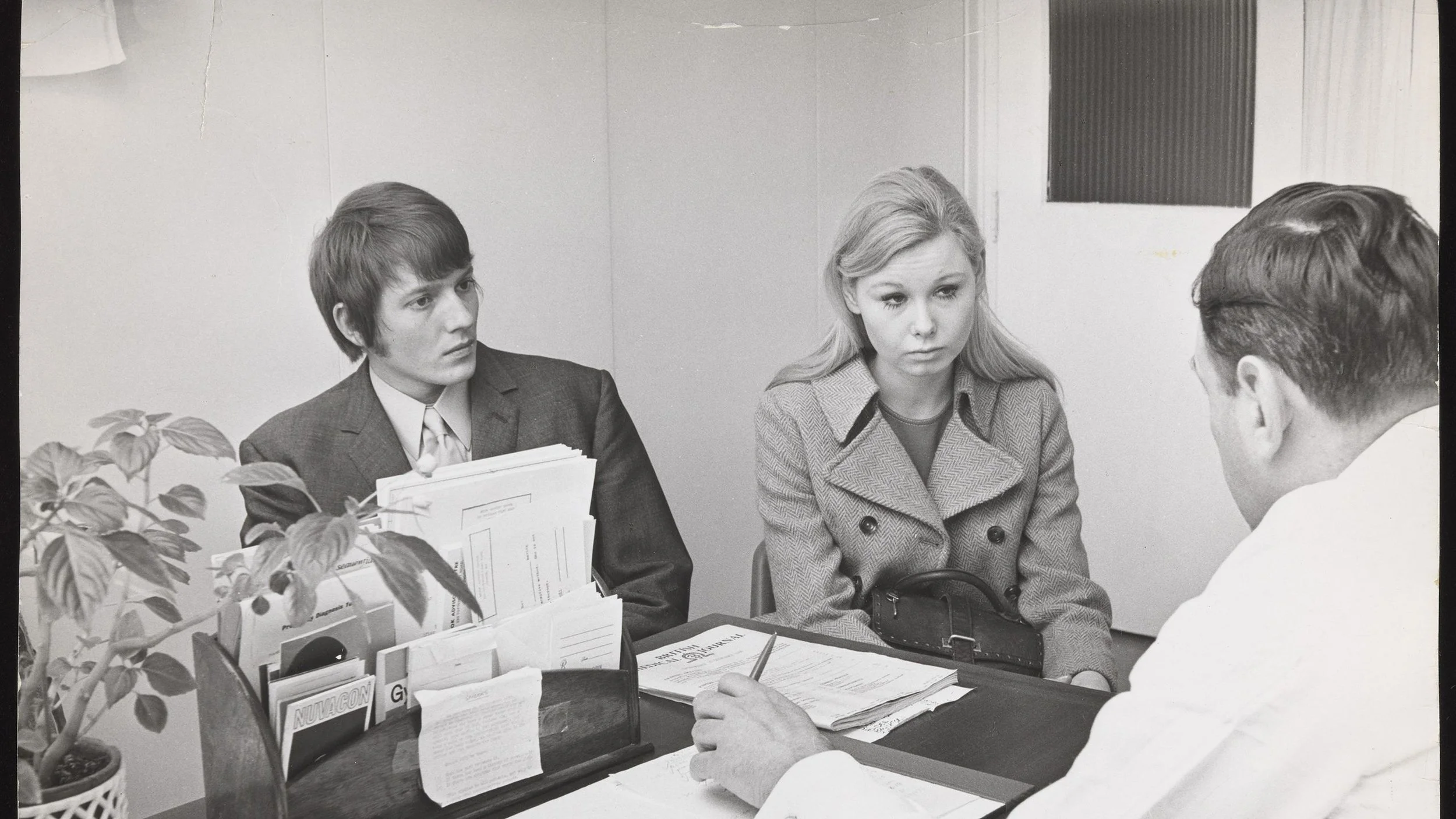
We can’t have a blog post about female pharmaceutical culture without spending some time on the contraceptive pill. It is often presented as one of the great liberating forces of the 1960s, a medical breakthrough that finally handed power to women. But was it really that simple? Was this the moment we moved away from the control of the 1950s and into an era of genuine reproductive freedom?
The oral contraceptive pill was officially launched in the UK on 4th December 1961 under the brand name Conovid. Approved by the British Family Planning Association and following clinical trials in Britain, it was hailed as a revolutionary development. Yet when Health Minister Enoch Powell (yes the very same) announced that the pill would be available through the NHS, there was an important catch: it would initially be available only to married women, specifically those who had already had children or whose health would be seriously threatened by another pregnancy.
So, from the very beginning, freedom came with conditions attached.
In practise, a married woman could not always simply decide to go on the pill. Access depended on the attitudes of individual male doctors, many of whom saw contraception as a matter that involved husbands as well as wives. In some cases, doctors actually required written permission from the husband before they would issue a prescription.
What followed was an intense political and social debate. Critics feared that expanding access would encourage ‘promiscuity’ and undermine traditional family values. In 1965, proposals to extend access to unmarried women were rejected outright. Just two years later, however, the NHS Family Planning Act 1967 transformed the landscape. For the first time, women could receive contraceptive prescriptions and advice regardless of marital status. This was genuinely revolutionary. For the first time in history, large numbers of women could separate sex from the constant anxiety of pregnancy. If women could choose if and when to have children, they could remain in education longer, delay marriage and even pursue long-lasting careers.
So all good, right?
Well, not quite. In fact, many of the tensions surrounding women’s healthcare today can be traced directly back to this moment, but I’ll save that for the “So What?” section.
There is also a tendency to assume that these changes rolled out uniformly across the UK when they did not. When Westminster passed the Family Planning Act, Scotland became a notable exception. William Ross, the Secretary of State for Scotland, actively blocked and delayed implementation for three years, arguing that Scotland was “not quite ready” for unmarried single women to access contraception. (Sigh.) Officially, this was presented as protecting Scotland’s “regional moral character”. In reality, it allowed politicians to avoid difficult conversations about female sexuality while postponing spending on reproductive healthcare.
The consequences were real. As historian Dr Kristin Hay has shown, many women learned to perform the role of the respectable, innocent woman simply to access contraception. Some unmarried university students reportedly wore fake wedding rings and lied to their GPs to avoid lectures, judgement or outright refusal. Meanwhile, sections of the Scottish press eagerly framed the pill as a moral crisis destroying Scottish values.
The 1960s promised a historic breakthrough in women’s autonomy, but the reality was far more complicated. In The Feminine Mystique, Betty Friedan challenged the idea that anatomy was a woman’s destiny. The pill could help women control their fertility, but it could not dismantle the structures of sexism that shaped their lives. A woman still couldn’t open a bank account without a male guarantor. She still faced significant barriers in education and employment. She still lived in a world designed around male authority.
It’s no surprise that Sylvia Plath’s The Ball Jar appeared in 1963. In one of its most famous passages, Esther Greenwood imagines her future as a fig tree, each branch representing a different life: marriage and children, a brilliant career, artistic success, travel, independence. Yet she feels unable to choose between them. As she hesitates, the figs begin to shrivel and fall. The pill may have expanded women’s choices, but choice itself could be paralysing when society continued to insist that women could not have everything at once.

1990s
In the 1990s, we start to see the emergence of a dual mindset when it comes to female pharmaceutical culture. Society became more willing to talk openly about mental health, while at the same time turning it into something that could be marketed, aestheticized and consumed.
By the 1990s, there had been a dramatic shift in how society viewed both mental health and body image, driven heavily by rapid pharmaceutical advances. Prozac became a cultural icon: the “It” drug of the decade. It redefined depression treatment as a more tolerable alternative to older antidepressants and became so influential that it inspired Elizabeth Wurtzel’s bestselling memoir Prozac Nation, which helped bring conversations about depression into the mainstream. Diet pills like Fen-Phen (fenfluramine and phentermine) fuelled a massive boom in the weight-loss industry, while Xanax skyrocketed in popularity for treating anxiety and became one of the most widely prescribed psychiatric medications in the US.
This created the perfect storm. The medical industry was providing pharmaceutical shortcuts at the exact same time the fashion industry was glorifying extreme thinness. Because the cultural goal was often to look “wasted,” frail or effortlessly skinny, some of the physical side effects of these drugs (dramatic weight loss, exhaustion and loss of appetite) could initially be interpreted as signs of success rather than warning signs.
However, while the 1990s helped destigmatise mental health by bringing it into public conversation, it simultaneously monetised and aestheticised the ‘unstable woman’ as a pop-culture trope. Greater visibility was not necessarily an invitation to accept the reality of psychological suffering. Instead, female pain was often transformed into another digestible, edgy and deeply gendered archetype: the beautiful, tragic, medicated girl.
You can see this contradiction perfectly captured in Girl, Interrupted (1999). The film offers two culturally distinct blueprints for female mental illness. Susanna represents the acceptable narrative: the palatable version of depression. She is quiet, observant, conventionally beautiful and ultimately compliant with her recovery. Then there is Lisa, the fetishised ‘cool crazy girl’, a blueprint that popular culture would return to again and again. She is charismatic, rebellious, and unpredictable, but also cruel, deeply damaged and ultimately unfixable. Audiences fell in love with this award-winning character, but only from behind a screen. She is the type of girl who is thrilling to watch for two hours, but not someone you would actually want to introduce to your parents.
The ‘cool crazy girl’ trope safely compartmentalised female suffering into a performance designed for external consumption. Mental illness was stripped of its unsexy realities (hygiene issues, cognitive decline and social isolation) and replaced by smudged eyeliner, hospital gowns worn like slip dresses and a detached cynical wit. In some ways, this echoes the 1950s. Then, a woman’s value was tied to her ability to endure suffering gracefully. By the 1990s, her instability was reframed as a sign of depth. The troubled woman became inherently more interesting than the ‘boring’ healthy one. Prescription medication became wrapped up in this identity. Carrying a bottle of Xanax or Prozac became a shortcut to looking complex, self-aware or rebellious. Medication was no longer simply something found in a suburban mother’s medicine cabinet; it increasingly became part of youth culture itself as a peer group rite of passage.
This shift transformed prescription pills from tools of adult conformity into a currency of teenage identity. Sharing a Xanax before a big exam or swapping a diet pill before a party became part of the cultural imagination of the decade: a shared coping mechanism for a hyper-competitive, image obsessed world. This was also the first generation of young people to be diagnosed en masse with conditions such as ADHD, depression and generalised anxiety. When an entire friendship group is visiting the school nurse for daily medication, the drugs begin to lose some of their clinical, intimidating, ‘grown-up’ aura.
The media quickly reflected this shift. Pills were no longer framed solely as an adult problem; they became a teenage lifestyle accessory. A teenager might hesitate before taking a powerful medication prescribed to an adult, but think nothing of accepting a colourful pill from a friend to calm their nerves before a date or help them lose weight before prom. Serious psychiatric intervention was transformed into something that appeared casual, social and even fashionable. And this happens again and again in 1990s media: Corey abusing diet pills in Empire Records (1995), Kathryn Merteuil carrying her drugs inside a silver crucifix necklace in Cruel Intentions (1999), or the teenagers in Nowhere (1997) casually navigating high school with a colourful assortment of pharmaceuticals always close at hand.
Present-Day
The 1990s laid the groundwork for the mid-2000s indie-sleaze era, epitomised by Effy Stonem in Skins. Effy was the direct evolution of the 1990s ‘unstable woman.’ She rarely spoke, smoked constantly and her severe psychological decline was heavily romanticised through a lens of teenage hedonism. By the 2010s and 2020s, prescription medication remained a recurring feature of teen dramas, appearing as a coping mechanism for the pressures young people faced, such as Spencer Hastings’ storylines in Pretty Little Liars. The ‘cool crazy girl’ trope also lived on through characters like Rue in Euphoria.
These characters become the ultimate fantasy of the damaged girl who could be saved, right up until her illness became too real, too disruptive or too ugly for the people around her to handle. You were allowed to talk about your depression, but only if you took your Prozac and remained a productive member of society. You were allowed to be "crazy," but only if your madness was visually appealing, sexualised or packaged as artistic angst.
And that brings us up to the present day.
With the rise of GLP-1 drugs like Ozempic and Mounjaro, we are once again witnessing a familiar pattern. These medications have been rapidly celebrated, rapidly condemned and endlessly debated. Is it any wonder that women no longer know which way to turn?
The cultural double standard surrounding prescription mediciation has never really disappeared; it has simply changed shape. Weight-loss drugs are often treated as acceptable, even aspirational through celebrity endorsement. Antidepressants can be framed as edgy, self-aware or part of carefully crafted identity. Anxiety, ADHD or bi-polar medication meanwhile, remain socially ‘shameful’. The categories shift, but the underlying question remains the same.
Which forms of female suffering is society willing to tolerate?
Looking back across the last century, a pattern begins to emerge. We tend to celebrate the mediacations that make women more palatable to society: thinner, calmer, more productive, more controllable. The medications that expose vulnerability, dependence or struggle are treated very differently. If the drug helps a woman conform to social expectations, we applaud it. If it reveals the cost of those expectations, we look away.
So What?
One of the most striking things about researching female pharmaceutical culture is how often the same debates keep resurfacing under different names. The drugs change, the marketing changes, the packaging gets sleeker, but the underlying conversations remain familiar.
For example, the aforementioned contraceptive pill is often celebrated as one of the greatest medical advances of the twentieth century, and rightly so. Yet many women will immediately recognise the frustration of having side effects dismissed, minimised or treated as an acceptable trade-off. Fast forward to today and similar debates surround every prescribed medication. Women are still routinely expected to weigh significant benefits against side effects that medicine often seems surprisingly comfortable asking them to tolerate (or prescribe them more pills to fix it!)
I can only describe this phenomenon as the ‘upper-downer cycle.’ In the 1950s, women were prescribed amphetamines to supress appetite and increase energy, but then needed barbiturates to help them sleep. By the 1990s, anti-anxiety medications and antidepressants often existed alongside diet culture and stimulant use. Today, we continue to live in a culture that demands productivity, thinness, emotional regulation and constant optimisation. It is perhaps no surprise that so many women find themselves taking one medication to function in the world and another to cope with the consequences of functioning in it.
There’s also the uncomfortable question of control. Across every decade in this article, the medications most enthusiastically embraced by society have often been the ones that make women more acceptable according to the standards of the time. This matters because we are still having these conversations. Women continue to be underdiagnosed with ADHD, PCOS and endometriosis, dismissed when reporting pain, scrutinised for taking antidepressants, judged for taking (or not taking!) weight-loss medication, and expected to navigate complicated decisions about hormonal contraception and its side effects. The tension that runs through this entire history remains unsolved.
Conclusion
So, looking forward, I can’t help thinking of those support phrases Instagram displayed before I even clicked on a single Ozempic video: “Know that your body is good enough.” “Take care of yourself.”
They’re lovely sentiments. The problem is that they exist alongside an endless stream of messages telling women the exact opposite.
Looking back across the last century, one thing becomes clear: women have repeatedly been offered pharmaceutical solutions to problems that were never entirely medical in the first place. The pressure to be thinner, calmer, prettier, more productive, more emotionally controlled or simply easier to manage has taken different forms across different decades, but it has never really disappeared.
I want to be clear that I am not demonising any of these medications. Every drug discussed in this this article has provided genuine benefits for millions of people. The contraceptive pill transformed women’s lives. Antidepressants have helped countless people navigate depression. Anxiety medication can be life-changing. For many people, drugs like Ozempic and Mounjaro may prove equally transformative.
The problem is not the medication.
The problem is the culture surrounding it.
History shows us that medication can be used to empower women, but is can also be used to reinforce expectations placed upon them. It can offer genuine relief while simultaneously allowing society to ignore the conditions that created the distress in the first place. Sometimes medication becomes a tool of freedom. Sometimes it becomes a way of helping women adapt to circumstances that perhaps should change instead.
If we genuinely want to improve women’s healthcare, then the conversation needs to extend beyond simply deciding whether a particular drug is “good” or “bad.” We need better research into side effects. We need to take women’s pain and health concerns seriously. We need to stop dismissing women when they report problems with medication, while also avoiding the moral panic that so often surrounds female pharmaceutical use.
Most importantly, we need to start asking harder questions about the pressures women are expected to navigate in the first place.
Because if generation after generation of women are being prescribed medication to cope with the same feelings of anxiety, exhaustion, inadequacy, overwhelm and dissatisfaction, then perhaps the most important question is not what women are taking. It’s why so many women feel they need to take it.
And that is a question no pill can answer.
Love this topic and want to explore more?
Things to look up:
The change from chemical control in service of national ideals (WW2 soldiers in Korea and Vietnam routinely given amphetamines) to modern zero-tolerance drug testing.
Racialised and moral framing around drug-use – middle class women were patients, other drug users are ‘addicts’.
The medical knowledge gap in female anatomy – menopause not a required topic for medical students until 2024/25.
Art piece ‘Just Take Ibuprofen’ by Emily Kampa.
1970 Nelson Pill Hearings
Watch:
Don’t Worry Darling (2022)
Girl, Interrupted (1999)
Empire Records (1995)
Cruel Intentions (1999)
Nowhere (1997)
Skins (2007)
Davina McCall's Pill Revolution (2023)
Valley of the Dolls (1966)
Read:
The Age of Anxiety: A History of America's Turbulent Affair with Tranquilizers by Andrea Tone
The Pope and the Pill: Sex Catholicism and Women in Post-war England by Dr Kristin Hay
The Feminine Mystique by Betty Friedan
The Bell Jar by Sylvia Plath
Prozac Nation by Elizabeth Wurtze
The Woman Destroyed by Simone de Beauvoir
Gender Trouble: Feminism and the Subversion of Identity by Judith Butler
Bonus Question to Think About!
If future medicine allows parents to choose more and more traits for their children, where should we draw the line between preventing suffering and designing a person?